
Introduction
Stereotactic body radiotherapy (SBRT) has become a standard treatment option for early-stage lung cancer and selected metastatic lesions, offering high local control with a limited number of fractions. However, the success of lung SBRT depends critically on geometric precision.
Unlike conventionally fractionated treatments, lung SBRT delivers large doses per fraction with steep dose gradients. In this context, inter-fraction motion—variations in patient and tumor position between treatment sessions—represents a major source of uncertainty. This article explores how rigid immobilization systems play a central role in minimizing inter-fraction motion and optimizing lung SBRT outcomes.
Why Inter-fraction Motion Is a Key Concern in Lung SBRT
Lung tumors are influenced by multiple sources of positional variability, including:
- Changes in patient posture and relaxation
- Day-to-day variations in respiratory pattern
- Tumor baseline shifts independent of breathing motion
- Differences in arm, shoulder, and thoracic positioning
While respiratory motion is often addressed through 4DCT, gating, or tracking, inter-fraction motion affects the baseline position of the tumor, potentially compromising target coverage if not adequately controlled.
The Distinction Between Intra-fraction and Inter-fraction Motion
In lung SBRT, it is important to distinguish between:
- Intra-fraction motion: tumor movement during beam delivery, primarily due to respiration
- Inter-fraction motion: changes in tumor position relative to external anatomy between fractions
Rigid immobilization primarily addresses the latter by ensuring that the patient’s overall body geometry is reproduced consistently at each treatment session.
Rigid Immobilization as a Foundation for Precision
1. Establishing a Reproducible Body Geometry
Rigid immobilization systems provide firm, indexed support for the torso, arms, and shoulders, reducing variability in thoracic posture.
Key benefits include:
- Consistent chest wall and rib cage positioning
- Reduced rotational and translational setup errors
- Improved alignment between simulation and treatment
By stabilizing the external anatomy, rigid immobilization indirectly stabilizes the internal tumor baseline position.
2. Reducing Setup Variability Across Fractions
Inter-fraction errors often arise from subtle differences in patient setup that are not fully corrected by image guidance alone.
Rigid immobilization:
- Limits degrees of freedom during setup
- Reduces dependence on large couch corrections
- Enhances the reliability of daily image registration
As a result, residual uncertainties after image guidance are minimized.
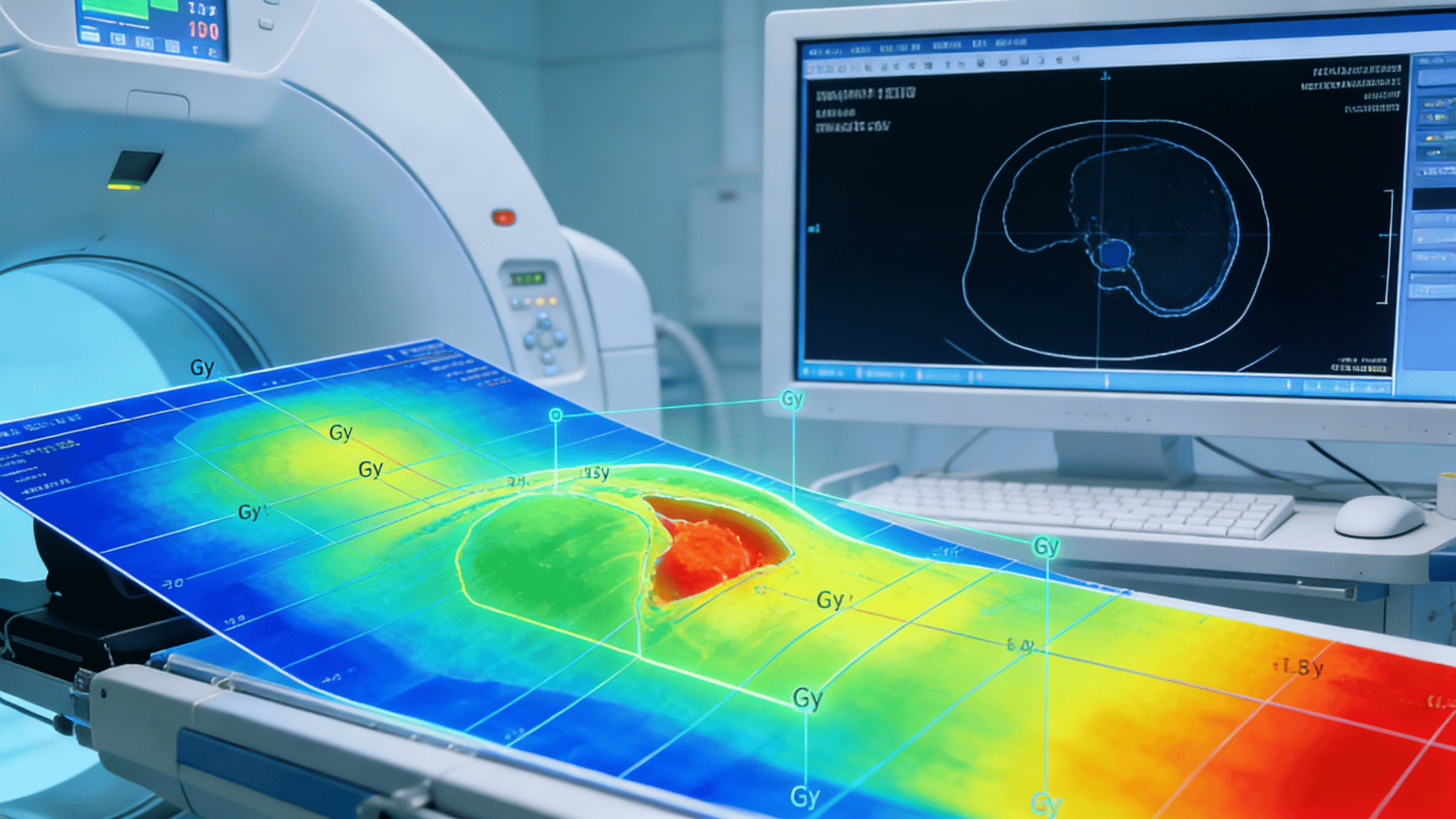
Impact on Target Margins and Dose Delivery
Reliable inter-fraction positioning enables clinicians to:
- Safely reduce PTV margins
- Maintain steep dose fall-off around the target
- Limit incidental dose to surrounding lung tissue, heart, esophagus, and spinal cord
In SBRT, where margins are intentionally small, even millimeter-level improvements in reproducibility are clinically meaningful.
Synergy with Image-Guided and Motion Management Techniques
Rigid immobilization does not replace motion management strategies such as:
- Respiratory gating
- Breath-hold techniques
- Real-time tumor tracking
Instead, it provides a stable reference framework that enhances the effectiveness of these technologies by reducing baseline variability.
When immobilization is poor, image guidance may correct translational shifts but fail to fully account for rotational or anatomical inconsistencies.
Clinical Benefits in Lung SBRT Practice
From a clinical perspective, improved inter-fraction stability contributes to:
- Higher confidence in target coverage
- Reduced normal lung dose and lower risk of radiation pneumonitis
- Greater consistency between planned and delivered dose
- Increased suitability for hypofractionated or dose-escalated regimens
These benefits directly translate into improved treatment quality and patient safety.
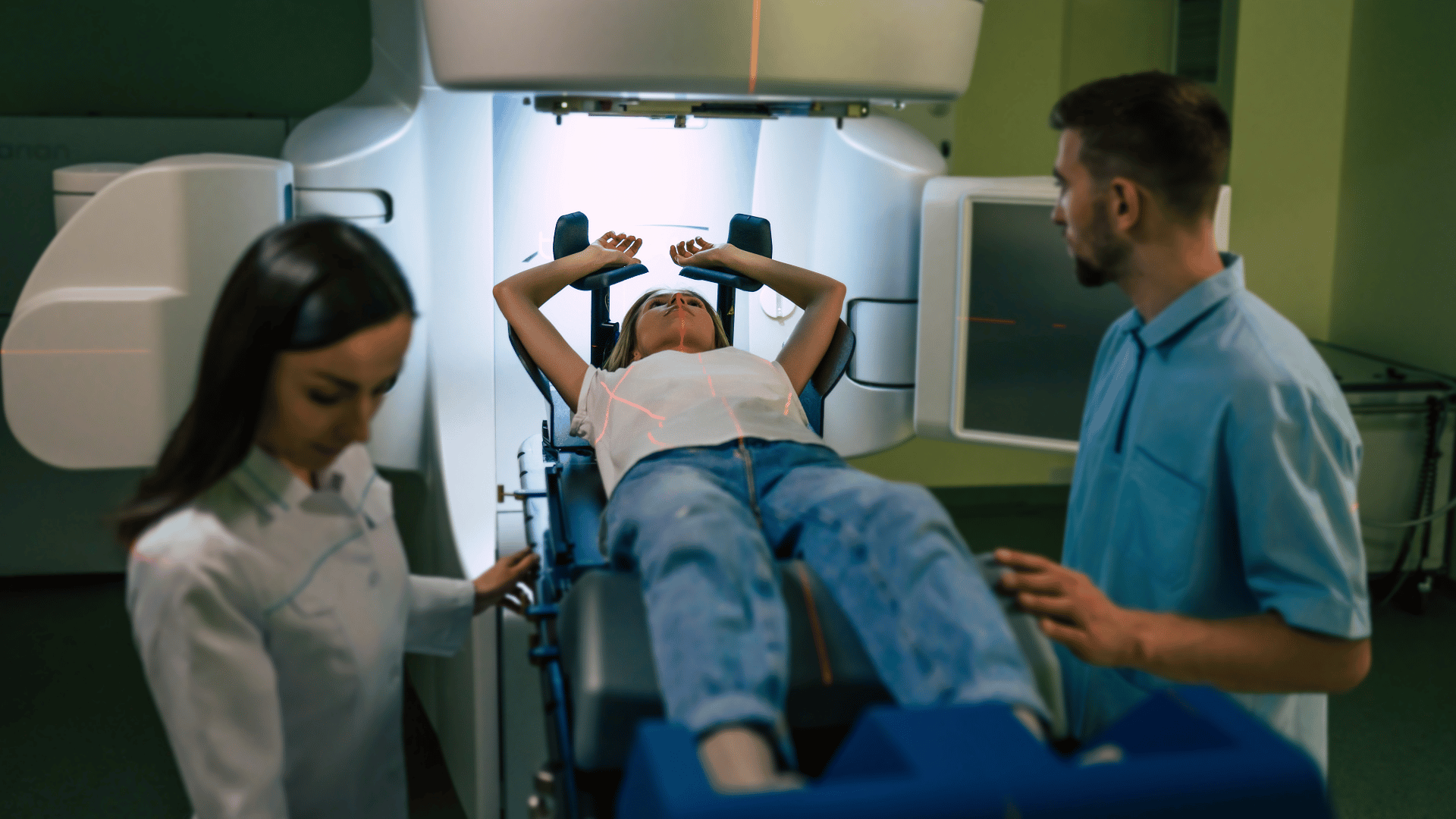
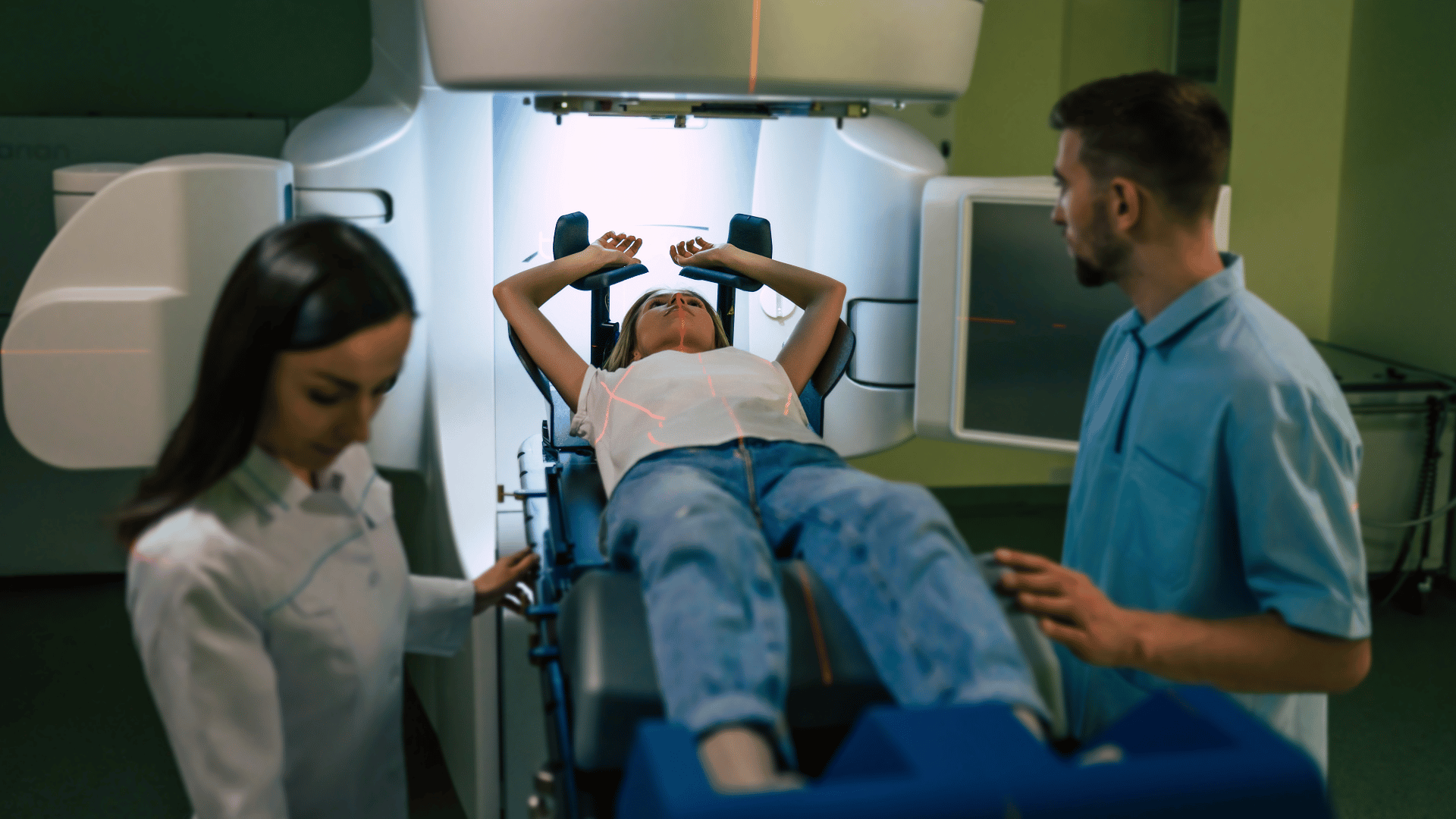
Patient Comfort and Compliance
Modern rigid immobilization systems are designed to balance stability with patient comfort. Secure yet ergonomic support reduces muscle strain and involuntary movement, helping patients maintain a consistent posture across all fractions.
Clear patient instruction and proper setup at simulation further enhance compliance and reproducibility.
Conclusion
In lung SBRT, precision is paramount, and inter-fraction motion represents a critical challenge to achieving optimal outcomes. Rigid immobilization systems play a fundamental role in minimizing this motion by ensuring consistent patient positioning across treatment sessions.
By reducing geometric uncertainty, enabling tighter margins, and supporting advanced image guidance, rigid immobilization forms the backbone of high-quality lung SBRT delivery—where accuracy is not just beneficial, but essential.