
Introduction
Radiotherapy for head and neck malignancies demands an exceptional balance between maximizing tumor control and protecting organs at risk (OARs). Structures such as the spinal cord, brainstem, parotid glands, optic apparatus, oral cavity, and larynx are often located only millimeters away from high-dose target volumes.
While modern planning techniques—such as IMRT, VMAT, and adaptive radiotherapy—have dramatically improved dose conformity, their clinical success is fundamentally dependent on geometric accuracy. Among the most influential yet sometimes underestimated contributors to this accuracy are advanced immobilization strategies.
This article explores how optimized immobilization directly supports OAR sparing in complex head and neck treatments and why it remains a key clinical concern for radiation oncologists.
Why OAR Protection Is Especially Challenging in Head & Neck Radiotherapy
Head and neck anatomy presents several unique challenges:
High density of critical structures within a confined anatomical space
Steep dose gradients adjacent to radiosensitive tissues
Inter-fraction anatomical changes, including weight loss, tumor regression, and edema
Intra-fraction motion, such as swallowing and subtle neck movement
Even small setup deviations can lead to clinically significant increases in OAR dose, potentially exceeding tolerance limits and increasing the risk of acute or late toxicity.
Immobilization as a Primary Tool for OAR Sparing
Although immobilization is often viewed as a technical prerequisite, it is more accurately described as a clinical risk-control measure. Effective immobilization minimizes systematic and random errors that would otherwise compromise OAR protection.
Key contributions of advanced immobilization include:
Reduced uncertainty in target and OAR positioning
Increased confidence in tight PTV margins
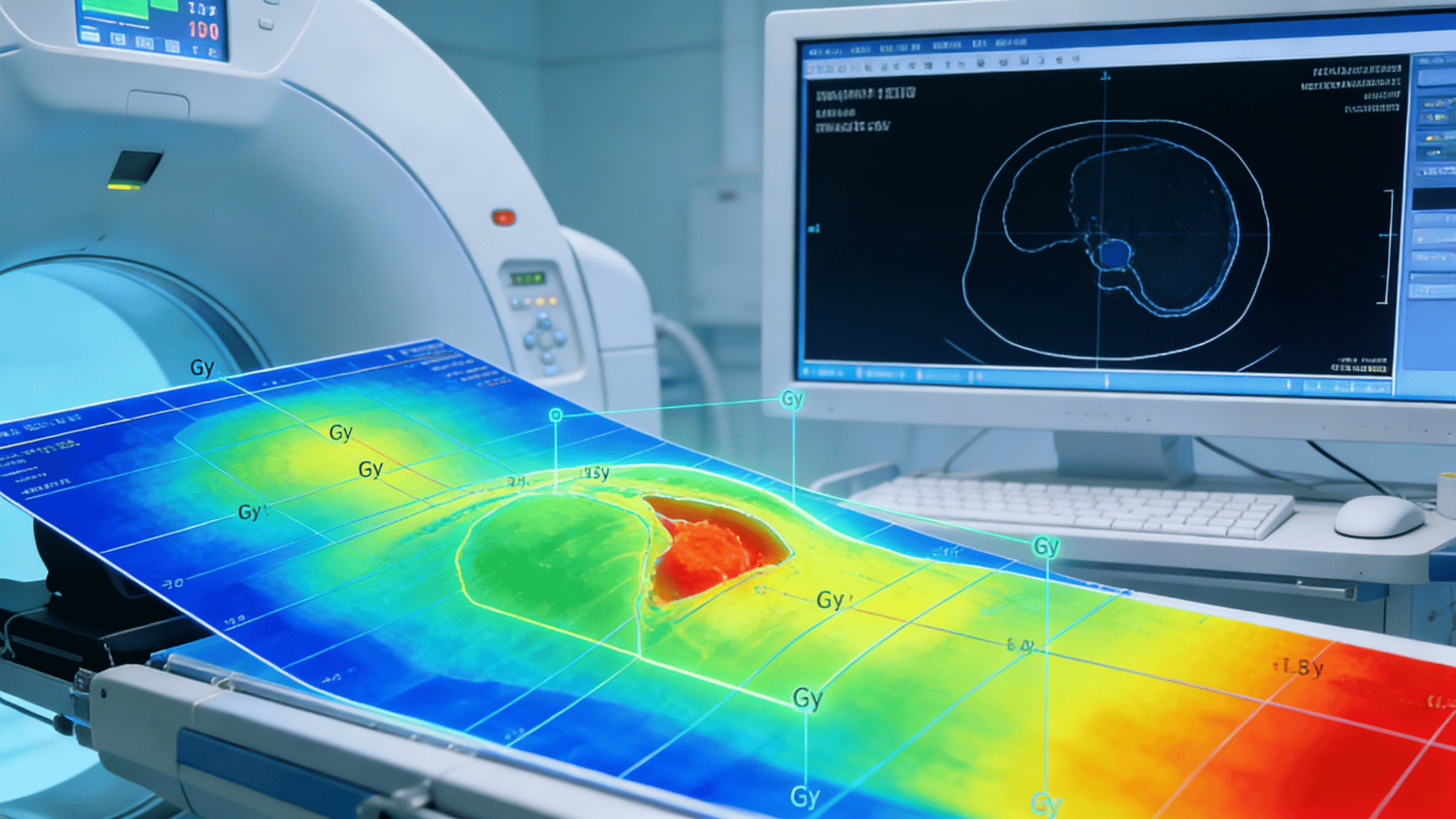
Improved reproducibility of planned dose distributions
Enhanced reliability of image-guided corrections
In essence, immobilization quality defines how closely the delivered dose matches the planned dose.
Advanced Immobilization Techniques for OAR Protection
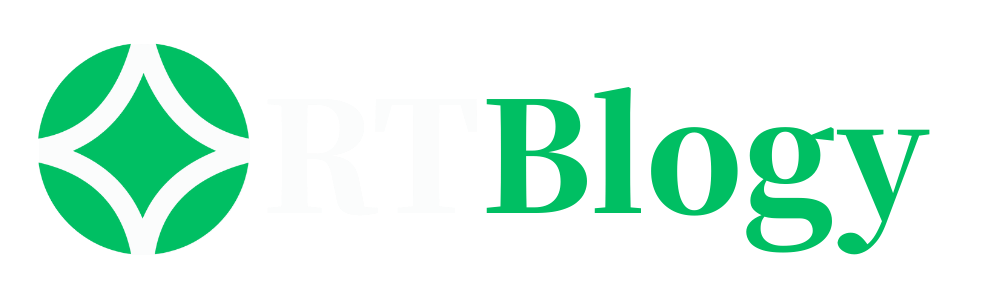
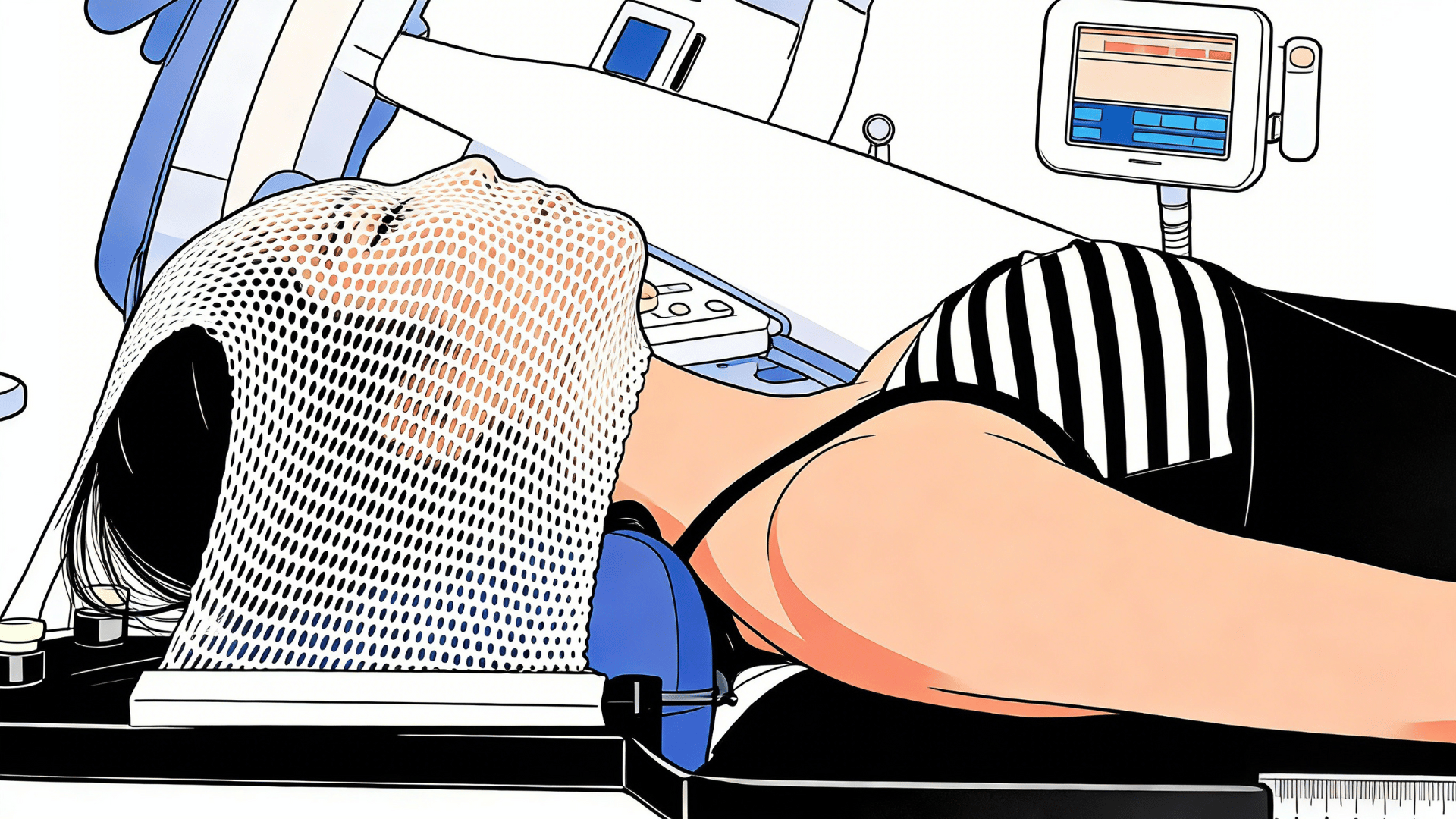
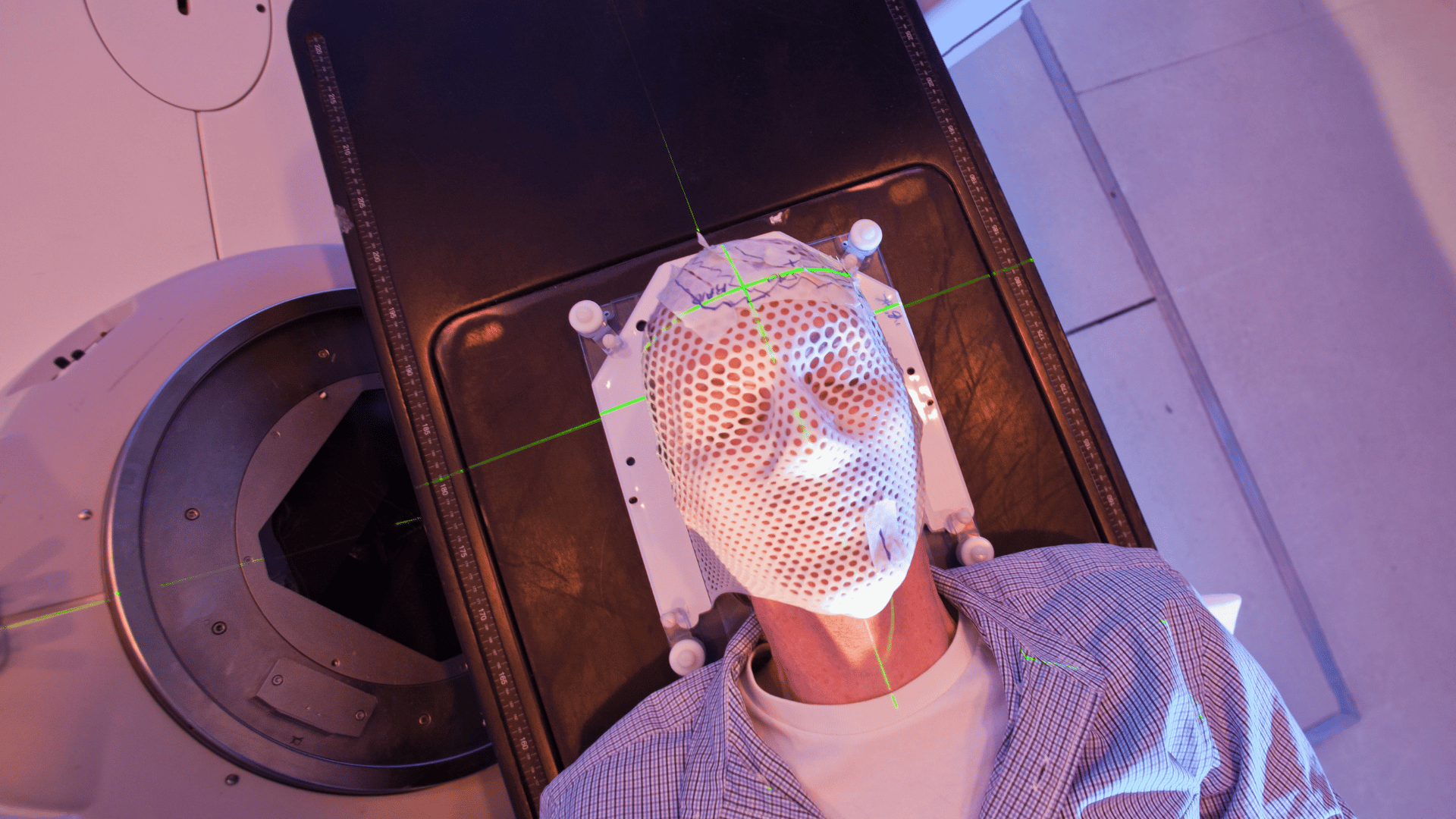
- High-Precision Thermoplastic Mask Systems
Modern thermoplastic masks are engineered to provide superior rigidity and anatomical conformity. When properly molded, they restrict both translational and rotational movement of the head and neck.
Clinical benefits include:
Improved spinal cord and brainstem sparing through consistent neck extension
Stable mandibular positioning to protect oral cavity and submandibular glands
Reduced day-to-day variation affecting parotid gland dose
Reinforced masks and multi-point fixation systems further enhance stability for complex cases.
- Customized Headrests and Neck Supports
Standardized headrests may not adequately accommodate individual anatomical variation. Customized supports help maintain consistent cervical spine curvature, which is particularly important when OARs such as the spinal cord or larynx lie close to high-dose regions.
By stabilizing the neck position, customized supports:
Reduce rotational uncertainty
Maintain spatial relationships between targets and OARs
Improve reproducibility across long treatment courses
- Bite Blocks and Intraoral Devices
In selected patients, bite blocks or intraoral stents provide additional immobilization and organ displacement benefits.
Their clinical impact includes:
Stabilization of the mandible and tongue
Physical separation of oral cavity structures from high-dose regions
Improved sparing of the tongue, oral mucosa, and salivary glands
When integrated with mask systems, these devices offer an added layer of geometric control.
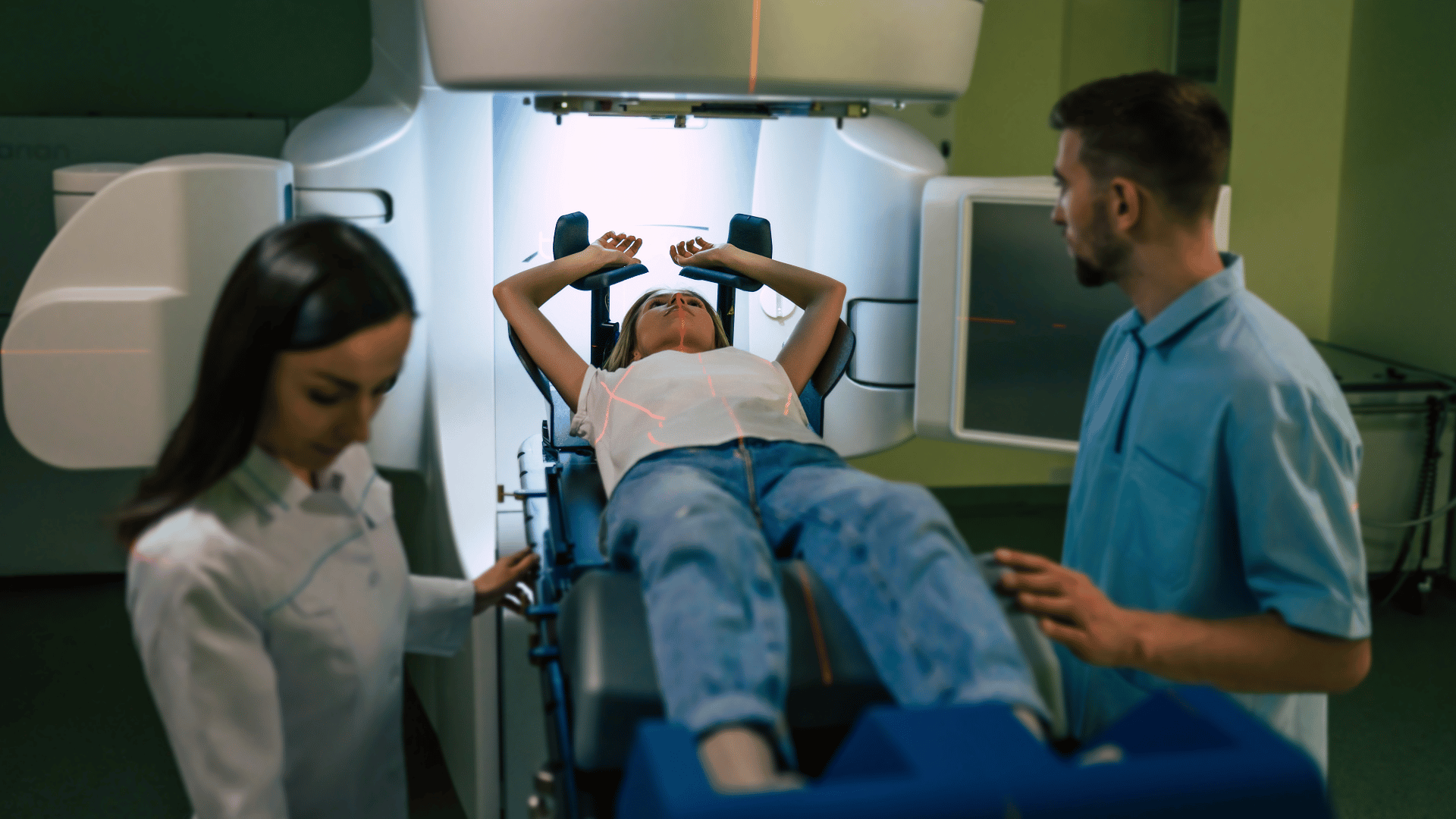
- Shoulder Immobilization and Extended Field Stability
For lower neck and supraclavicular targets, shoulder position can significantly influence dose distribution. Shoulder pull systems or indexed arm supports help prevent superior shoulder migration into high-dose regions.
This is particularly relevant for protecting:
Brachial plexus
Lower cervical spinal cord
Inferior pharyngeal structures
Immobilization and Margin Reduction Strategies
One of the most direct links between immobilization and OAR protection is margin management. Reliable immobilization allows clinicians to safely reduce PTV margins without increasing the risk of geographic miss.
Smaller margins translate to:
Lower incidental dose to nearby OARs
Reduced integral dose
Enhanced therapeutic ratio
Without robust immobilization, margin reduction becomes clinically unsafe, regardless of planning sophistication.
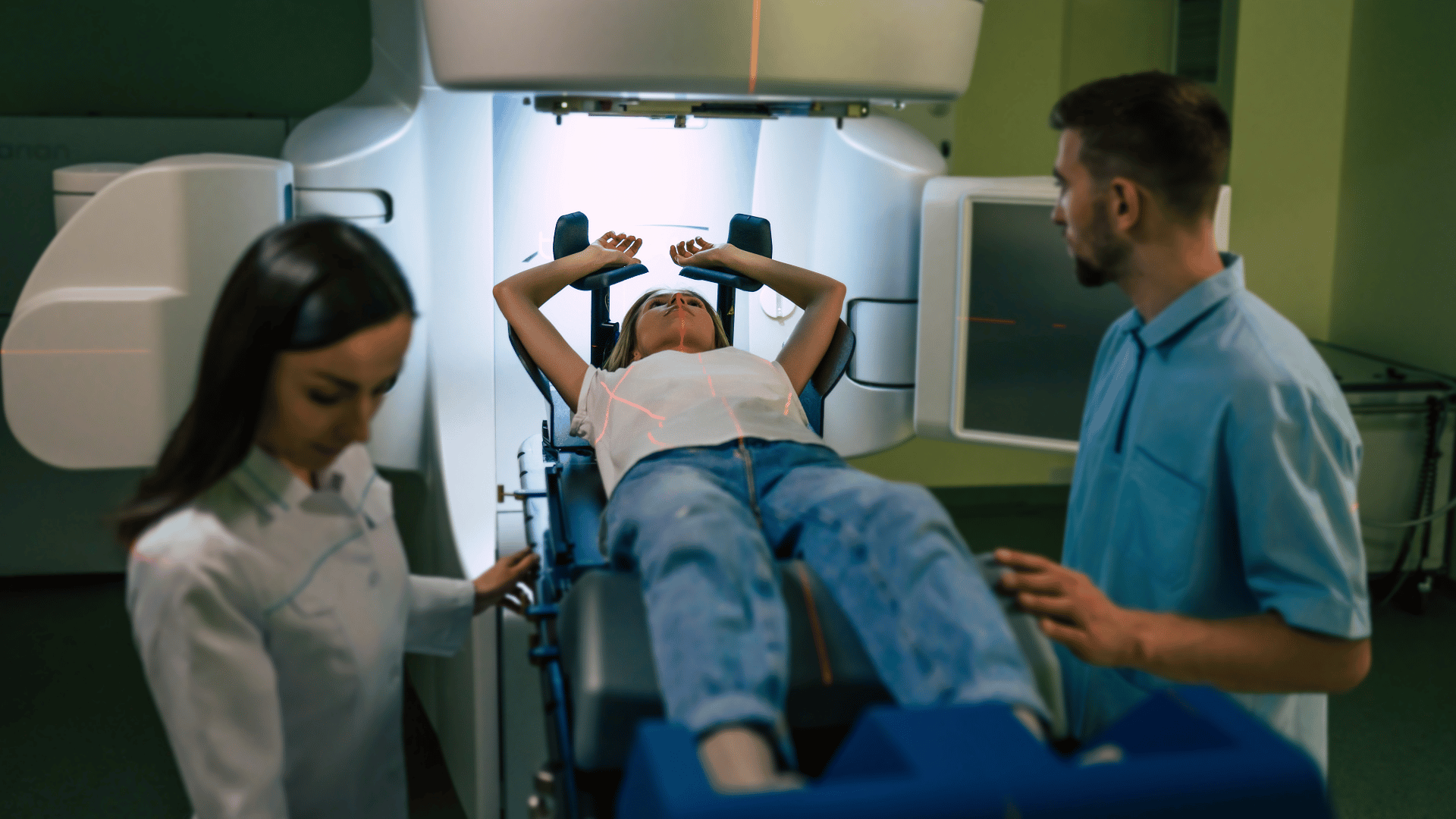
Synergy with Image-Guided and Adaptive Radiotherapy
Advanced immobilization does not replace IGRT or adaptive strategies—it enables them.
High-quality immobilization:
Improves initial setup accuracy, reducing large daily corrections
Enhances the reliability of deformable image registration
Supports adaptive replanning decisions based on true anatomical change rather than setup variability
For physicians, this synergy is essential for maintaining OAR dose constraints throughout treatment.
Clinical Perspective: What Matters Most to Physicians
From a clinical standpoint, immobilization quality directly influences:
Confidence in spinal cord and brainstem maximum dose
Parotid gland mean dose consistency
Predictability of toxicity outcomes
Willingness to adopt advanced techniques such as dose escalation or hypofractionation
In complex head and neck cases, immobilization is not simply a technical detail—it is a clinical safeguard.
Conclusion
Protecting organs at risk in complex head and neck radiotherapy requires more than advanced planning algorithms. It demands a comprehensive approach in which advanced immobilization strategies play a central role.
By ensuring consistent patient positioning, minimizing geometric uncertainty, and enabling tighter margins, high-quality immobilization directly supports the primary clinical goal shared by every radiation oncologist: maximizing tumor control while minimizing harm to critical normal tissues.
As treatment complexity continues to increase, the importance of immobilization as a tool for OAR protection will only grow.

{kind=link}
{kind=link}